Who is Thomas Massie (R-KY) and why is he the only Republican who voted against U.S. House Resolution 246 (Opposing efforts to delegitimize the State of Israel and the Global Boycott, Divestment, and Sanctions Movement targeting Israel)?
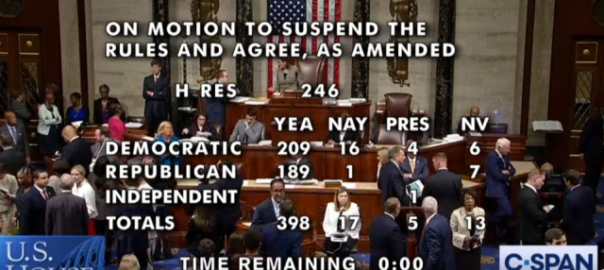
H.R. 246, in a non-binding resolution approved 398–17, condemns the movement to boycott, divest and sanction (BDS) Israel for its policies regarding the Palestinians. Who says bipartisanship is dead? When it comes to pissing on Palestinians, Democrats and Republicans have no trouble coming together.
The resolution, backed by the American Israel Public Affairs Committee, also enshrines the long irrelevant two-state-solution to the Palestinian-Israeli conflict, in a presumably sharp rebuke of current Trump administration and Israeli policy.
Additionally, H.R. 246 says Americans have a “right to petition in opposition to government policy,” soothing some Democrats who oppose a stronger Senate anti-BDS bill that penalizes companies and individuals for supporting boycotts, divestment or sanctions directed towards Israel.
Massie ignored the rhetorical smoke screen and recognized H.R. 246 for what it was — a government-led effort to discourage the exercise of free speech. If only more Democrats looked upon the Constitution with the same respect Massie does.
Massie, an M.I.T. grad, is the kind of ‘maverick’ politician other ‘maverick’ politicians keep at arm’s length. He is both predictable and hard to predict. An unfailing anti-interventionist and strong deficit-hawk since entering Congress in 2012, Massie was endorsed by former Texas Representative Ron Paul and his son Kentucky Senator Rand Paul.
He’s the male Tulsi Gabbard (D-HI), skeptical of U.S. strategy in the Middle East and the hundreds of other military commitments spread throughout the globe. In May, with Congressman Andy Levin (D-MI), he introduced the Authorization for Use of Military Force (AUMF) Clarification Act, designed to require the Trump Administration to receive an explicit authorization from Congress before engaging in military action against Iran.
“Article I, Section 8 of the U.S. Constitution clearly gives Congress the sole power to declare war,” Massie said. “Our Founding Fathers believed that Congress — not the President — should possess this power, and that giving such authority to the executive branch presents a direct threat to liberty. As the AUMF Clarification Act states, Congress has never authorized military force against Iran, and any such action would be illegal and unconstitutional without an up-or-down vote.”
The AUMF Clarification Act argues that the 2001 Authorization for Use of Military Force, the Authorization for Use of Military Force Against Iraq Resolution of 2002, nor any other existing law gives the Trump administration the legal authority to use force against Iran. Only a direct authorization by the Congress would give the administration authority.
Not surprisingly, the Trump administration points on current Iran policy, National Security Adviser John Bolton and Secretary of State Mike Pompeo, disagree.
Both Gabbard and Massie don’t blindly cheerlead U.S. military adventurism lacking sufficient predicate or well-defined goals. However, since he’s not a woman, Massie doesn’t get smeared as being soft on dictators and tyrants as Gabbard does. He’s ‘thoughtful’ and ‘highly-principled’ according to his congressional colleagues, while Gabbard is ‘weak’ and easily “manipulated” by totalitarian rulers, according to her fellow Democratic Party critics. If you ever want examples of palpable sexism and bias, spend just a few days listening Democrats talk about other Democrats.
Which is why H.R. 246 has been a disturbing outcome for many progressives who fight for the human rights of Palestinians living under Israeli occupation or substantive control. What made the House vote on H.R. 246 so striking is that Massie was on the only Republican to vote against it, while Gabbard and most progressive Democrats, to the dismay of many of their supporters, voted in favor.
Independent journalist and documentary filmmaker Abby Martin, whose film “Gaza Fights for Freedom” was released in June, didn’t hesitate to call out the rank hypocrisy of progressives with respect to H.R. 246:
Ro Khanna (D-CA) and Ayanna Pressley (D-MA) spent a good part of Wednesday on Twitter explaining their ‘yea’ votes to constituents and followers:
If groveling contrition were an Olympic sport, Khanna and Pressley just won the gold and silver in the ‘How to Betray Palestinians While Pretending You are Their Biggest Supporter.” Spare us your mental gymnastics Ro and Ayanna.
When the U.S. government criticizes free speech (e.g., boycotts) — even without legislating against it — it is discouraging free speech. As a First Amendment-hawk, Massie didn’t need to parse out political considerations from his principles, He knew how to vote on H.R. 246.
And accusing Massie of anti-Semitism over this vote would be like calling Santa Claus the Grinch that stole Christmas. The accusation would never stick. He has no ill-expressed criticisms of Israel that can be misinterpreted as anti-Semitic or any other kind of demonstrable religious, racial or ethnic bias. He criticizes policies, not people, religions or countries.
Unfortunately, for many Democrats, the fear of such a charge has led them down a dark path that not only chips away at our Constitutional freedoms, but makes it increasingly likely that the U.S. will get involved in a prolonged military action against Iran at the urging of the Israeli and Saudi Arabian governments — just one more military commitment to add to our current participation in conflicts in Syria, Iraq, and Yemen.
But what is most problematic about support for H.R. 246 is that it normalizes anti-BDS sentiments — including the association of pro-Palestinian activists as anti-Semitic hate groups on par with the neo-Nazis and KKK — and clears the path for more draconian anti-BDS legislation to become law at the state-level.
While 16 Democratic House members voted against H.R. 246, including Alexandria Ocasio-Cortez (D-NY), Rashida Tlaib (D-MI) and Ilhan Omar (D-MN), Massie may be the lone North Star in the Republican Party, along with the few remaining in the Democratic Party, still pointing us towards the protection of our constitutional freedoms and recognizing the human rights and dignity of the Palestinian people.
K.R.K.
Send thoughts and criticisms to: kroeger98@yahoo.com
When presented with complex or too much information, willful ignorance often feels like the best option.
“If the cost of educating oneself outweighs the benefit of obtaining deeper or more accurate information, then it is rational to simply ignore contradictory inputs,” argues Kathleen Schaefer in the Journal of International Service. “Economists describe this acceptance of narratives at face value as part of rational ignorance.”
Schaefer’s focus was immigration, but her words just as easily apply to the U.S. healthcare system. Constituting almost 20 percent of the U.S. economy, few issues are as complex as healthcare.
Indeed, it is that narrative about ‘health care policy being too complex for easy solutions’ that is keeping good policy ideas from being embraced by otherwise competent political, news media and economic elites.
Rational ignorance loves the status quo or, if forced, the adoption of incremental policy changes — policies such as Obamacare.
So when former Vice President Joe Biden says of Bernie Sanders’ Medicare-for-All plan that “all the Medicare you have is gone. It’s a new Medicare system. It may be as good, you may like it as well, it may or may not, but the transition of dropping 300 million people on a totally new plan, I think is a little risky at this point.”
Biden is putting on display his own rational ignorance — and it is not just him. A recent MSNBC panel discussion hosted by Stephanie Ruhl kept throwing out terms and phrases like “risky,” “too costly,” “starting from scratch,” and “revolutionary” to describe Sanders’ plan, and calling Biden’s proposal to build off of Obamacare and offer a public option as “safe,” “reasonable” and more “achievable.”
In fact, the opposite may be true and to understand why it important first to understand the gravity of the problems facing our current U.S. healthcare system.
The U.S. healthcare system is broken
No matter how many times Fox News’ Sean Hannity says “the U.S. has the best healthcare system in the world,” it doesn’t make it true. To the contrary, the U.S. healthcare system is a significant outlier among other advanced economies — but not in a good way.
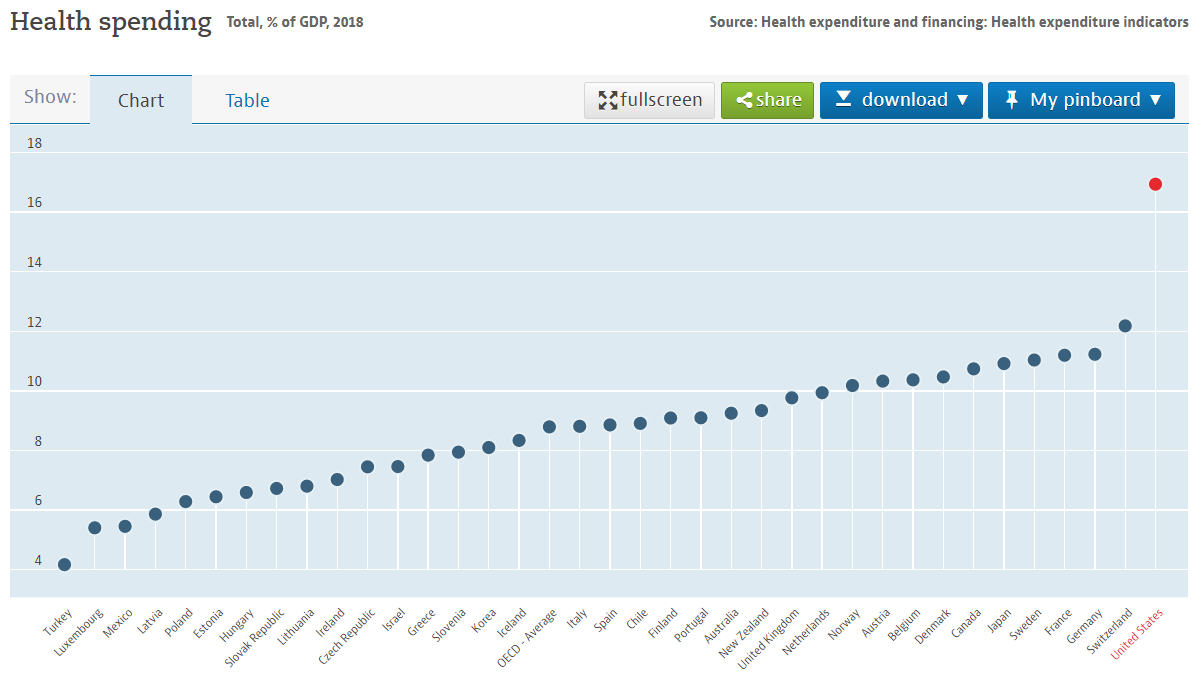
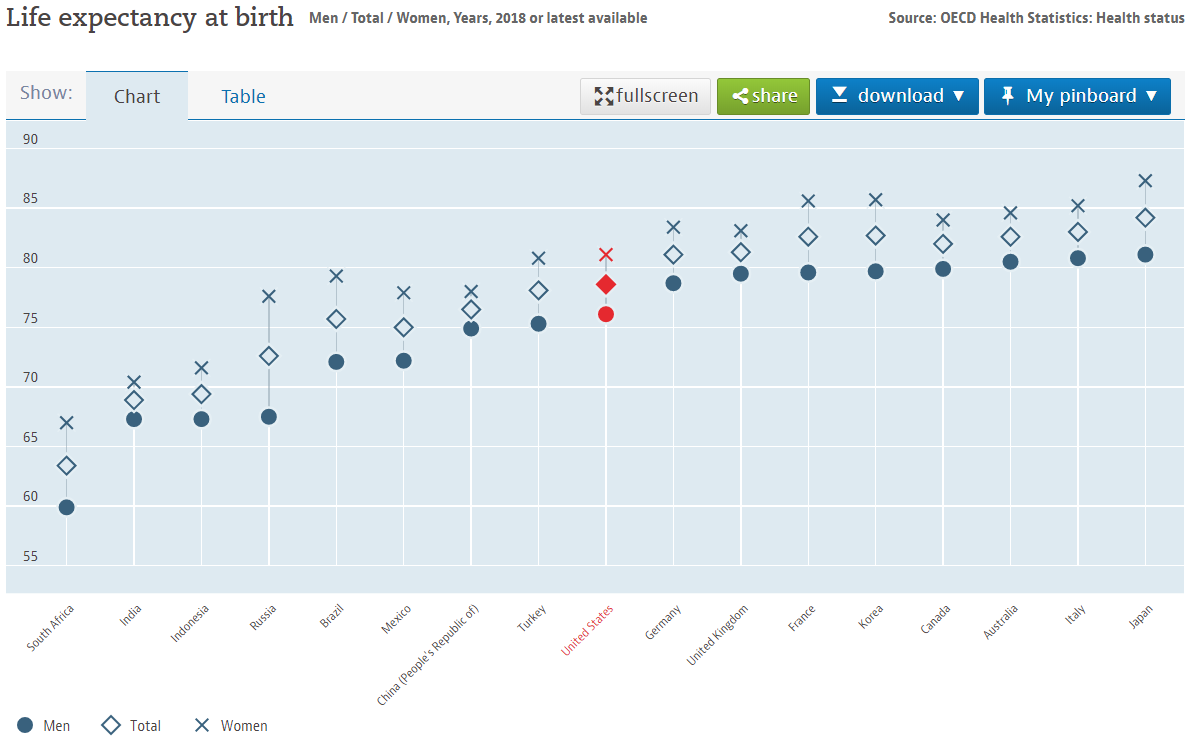
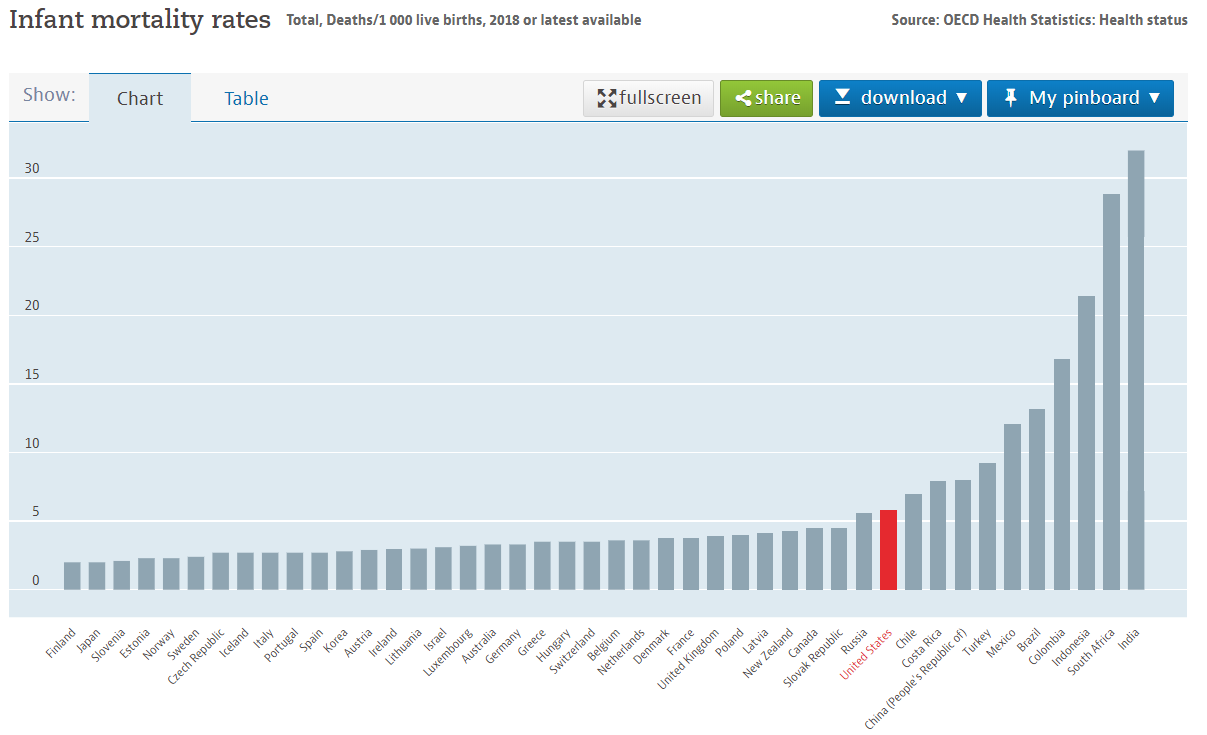
Americans pay twice as much for healthcare (Figure 1), yet, in the aggregate, achieve markedly inferior health outcomes. For example, we die younger (Figure 2) and have a higher infant mortality rate (Figure 2) than most other advanced economies.
Figure 1: Health spending as a % of GDP (Source: OECD, 2018)
Figure 2: Life expectancy at birth (Source: OECD, 2018)
Figure 3: Infant mortality rates for selected countries (Source: OECD, 2018)
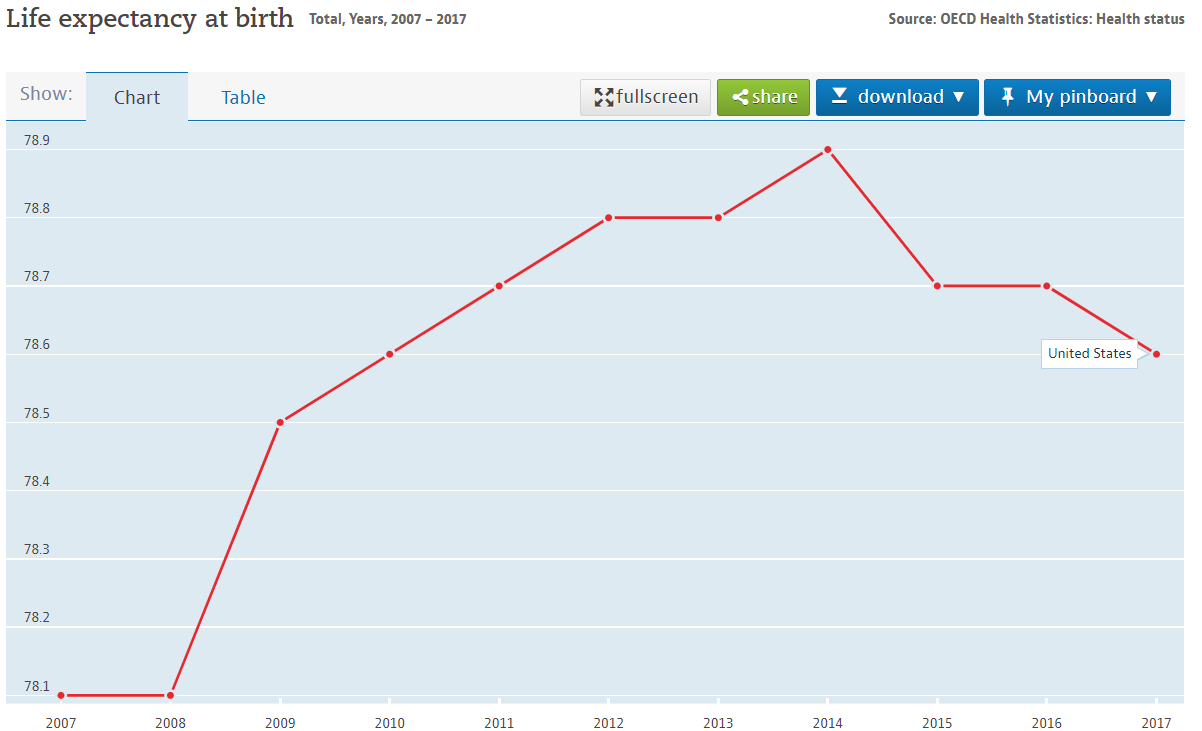
Figure 4: Trend in life expectancy at birth in the U.S. (Source: OECD, 2017)
These statistics are not the result of an analytic sleight-of-hand. They are straightforward metrics long measured and commonly used for cross-national comparisons. And the conclusion drawn from them is unmistakable: the U.S. healthcare system underperforms relative to other advanced economies.
Why?
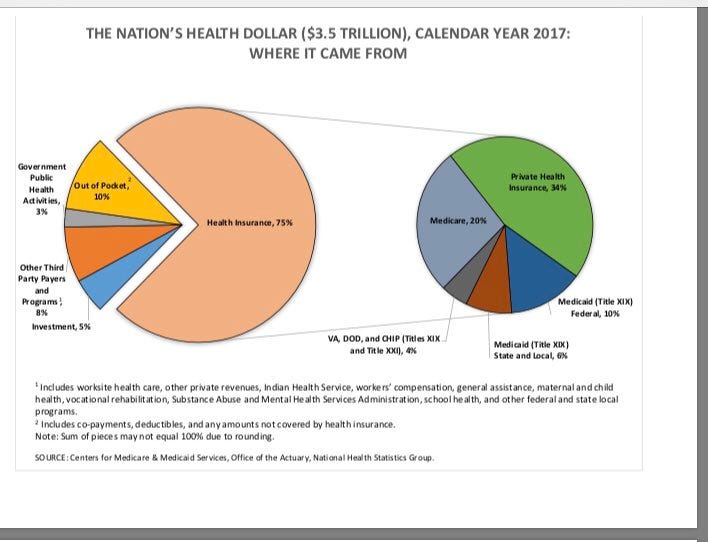
The reasons are many and better described elsewhere, but health economists generally agree that one reason is the U.S. private insurance industry adding a layer of administrative costs not present (to the same degree, at least) in most other advanced economies. The Centers for Medicare and Medicaid Services (CMS) estimate the U.S. private insurance industry accounts for 34 percent of the health insurance dollars (Figure 5) — which translates to nearly $1 trillion.
Figure 5: The Source of U.S. Healthcare Dollars
And while private insurance’s share of the health insurance dollars will likely decline as the U.S. population ages, their financial bottom line will not necessarily suffer if recent performance is an indicator. According to Berkshire Hathaway, through third-quarter 2018, health insurers’ net income grew by 19 percent to $25.8 billion compared with the same prior-year period. Zacks Equity Research reports that the private health insurance industry generated returns higher than the S&P 500 index in each year from 2012 to 2017, returning an impressive 257 percent compared with the S&P 500 index’s gain of 91 percent. This is a good time to be the health insurance industry.
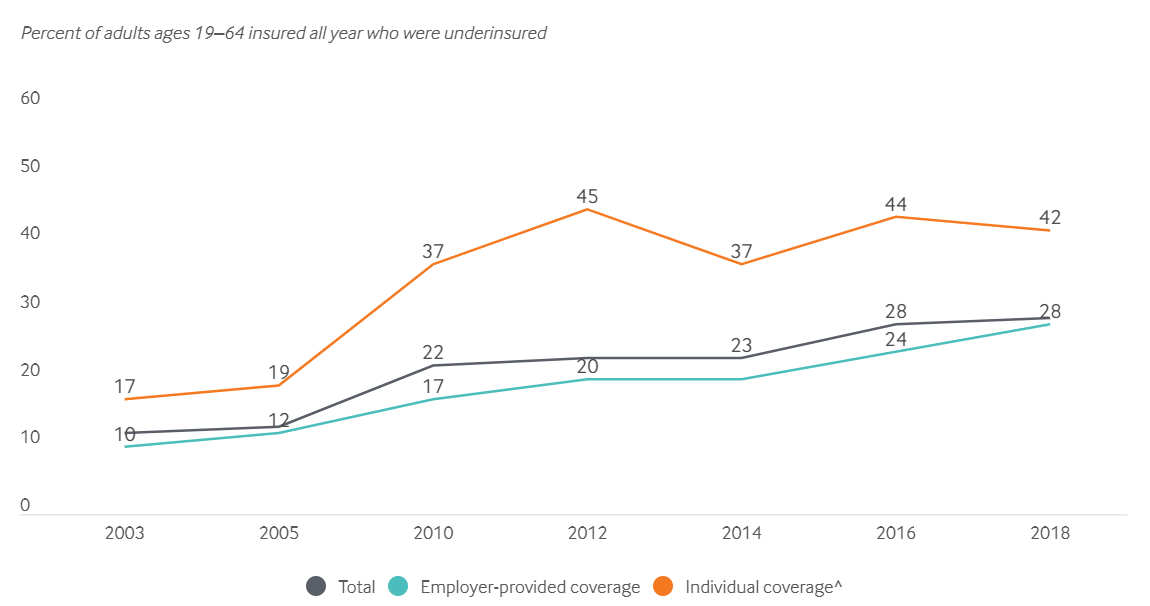
It is not, however, a good time to need medical care. While the Affordable Care Act (“Obamacare”) significantly reduced the percentage of Americans without insurance from 18 percent in 2013 to 11 percent in 2016, that percentage has since risen to almost 14 percent in late 2018, according to the Gallup Organization. In addition, The Commonwealth Fund recently reported that the percent of underinsured American adults (aged 19–64) has risen from 10 percent in 2003 to 28 percent in 2018 (Figure 6).
And for those Americans with private health insurance — either through their employer or through an individual plan — costs have risen prohibitively over the past 20 years. In 2018 the average annual premium for employer-based family coverage was $19,600 (up 5 percent from 2017) and was $6,900 for single coverage (up 3 percent from 2017), according to the National Conference of State Legislatures. In 1999, the average annual premium for family coverage was only $6,000, and for single coverage around $2,500.
There is only one rational conclusion: The U.S. healthcare system is under-delivering, whether in comparison to other advanced economies or to its own past performance.
The media, politicians, and Sanders himself are misrepresenting Medicare-for-All
In this context, Sanders’ Medicare-for-All plan is hardly ‘revolutionary,’ ‘radical’ or a ‘fundamental transformation’ of the U.S. healthcare system. It takes an existing, successful public health program — Medicare — and, over time, expands it to the remaining segments of the population.
But its critics drive home a contrasting picture of Medicare-for-All:
Medicare-for-All requires starting from scratch!
As seen in Figure 5 above, public health programs (Medicare/Medicaid, CHIPs, DoD’s Tricare, the Veterans Administration healthcare system) already account for two-thirds of U.S. health insurance dollars and, even without Medicare-for-All, will likely increase its share over time as the American population ages. And with the rapid advancement of artificial intelligence and machine learning, scaling up the current Medicare system to the rest of the population should become easier. Medicare-for-All is the exact opposite of starting from scratch.
It’s too expensive!
Medicare-for-All critics also instill doubt by suggesting the program’s expansion will lead to substantially higher taxes and potentially national bankruptcy. Sanders’ senior economic advisor, economist Stephanie Kelton, has a direct response:
Most estimates of Medicare-for-All’s costs over its first 10 years range from $32 trillion to over $40 trillion. Yes, that is a big number, but remember that our current healthcare system is going to cost between $34 trillion and $47 trillion.
Any forecast about healthcare spending is built upon debatable assumptions, but, at a minimum, we should be able to answer with confidence, “Will Medicare-for-All increase or decrease healthcare spending overall?”
Based on Sanders’ description of his Medicare-for-All plan, cost savings will occur in four primary areas: (1) reduced drug prices through increased price competition, (2) reduction in administrative costs (i.e., elimination of private health insurance), (3) constraints on provider payment rates (i.e., what doctors and hospitals are paid), and (4) increased use of preventive medicine (resulting in a healthier population and less demand for high-cost medical services).
Forecasts on Medicare-for-All costs are sensitive to assumptions, particularly regarding whether or not Medicare-for-All will pay current Medicare/Medicaid rates (which are generally below actual costs).
Assuming Medicare-for-All reimbursement rates remain near current Medicare/Medicaid rates, the real problem with Medicare-for-All is that it shrinks 20 percent of the U.S. economy.
How will economic growth be affected, particularly in the short-term, if cost rationality is brought to our healthcare system? How do you eliminate an entire industry (supplemental, private-based insurance notwithstanding) and not cause a recession?
As described by the Sanders campaign, Medicare-for-All is more likely to put downward pressure on what this country spends on healthcare.
It will require the government to raise taxes on the middle class!
Similarly, the claim that middle class taxes will rise under Medicare-for-All dovetails with the ‘too expensive’ argument and rests on the same question: Can we achieve total cost savings through Medicare-for-All?
Regrettably, Bernie Sanders didn’t help his cause by telling the Associated Press that his healthcare plan could cost up to $40 trillion over a decade and that he’d consider raising taxes on the middle class “in exchange for healthcare without co-payments or deductibles.” Lost in the translation is that Sanders believes the savings to households by eliminating co-payments and deductibles would exceed any tax hike.
Still, he did say he’d consider raising middle class taxes and that is all his critics needed to hear.
Setting aside the distinction between families sending their money to insurance companies through payroll deductions, deductibles and copays versus paying a healthcare tax, the probability of tax increases pivots on whether Medicare-for-All can reduce costs.
If ‘yes,’ then the Medicare-for-All tax will merely be replacing premiums, deductibles and copays and perhaps even leave households more disposable income. If ‘no,’ then tax increases will be necessary — and taxing the rich probably won’t be enough if Medicare-for-All cost estimates by Urban Institute healthcare analysts John Holahan and Linda J. Blumberg are accurate. They estimate Medicare-for-All over 10 years will cost $33 trillion and will be entirely financed by taxes on individuals and businesses. Even research by the Mercatus Center, a libertarian think tank funded by the Koch brothers, assessed that Medicare-for-All could save $2 trillion in total spending, costing around $32 trillion over a 10-year period.
Predictably, Joe Biden has picked up on this area of disputatiousness within Sanders plan and is declaring that “Bidencare” — in contrast — will expand healthcare coverage and lower costs without raising taxes on the middle class (the details on how he will do that are still pending). The Biden attack on Medicare-for-All has also been reinforced by the news media, with the Washington Post poo-pooing the Mercatus Center savings conclusion as being cherry-picked from that study.
So why am I not convinced that Medicare-for-All will lead to higher healthcare-related spending by households?
There is one incontrovertible fact that the American news media, policy analysts, business lobbies and political class continue to ignore: Every advanced economy with universal coverage delivers better healthcare to their citizens and does so at a unit cost significantly lower than the U.S. (see Figure 1 above).
Germany does it. France does it. Canada does it. The United Kingdom does it. Japan does it. And there is no inherent reason the United States can’t do it, if the political will exists to do so.
Many of these countries pay higher tax rates than Americans, but that does not explain why they deliver healthcare at lower cost and with superior outcomes.
As taxpayers, we should fight paying higher taxes for healthcare as long powerful special interests groups co-opt our healthcare system, bloating its costs for exorbitant private gain and leaving Americans in significantly poorer health than comparable populations in other countries.
The ‘middle class tax increase’ canard is a distraction with one purpose: scare Americans away from thinking a single-payer healthcare system is possible.
But it is possible. California Representative Ro Khanna recently responded to Biden’s tax increase criticism by noting that if the healthcare status quo persists it will cost us $49 trillion over the next 10 years. If Medicare-for-All were to come anywhere close to the $32 trillion price tag estimated by the Mercatus Center and The Urban Institute, middle class Americans won’t be worrying about a tax increase, but rather how to spend the money they’ve saved under Medicare-for-All.
It’s socialized medicine that will lead to healthcare rationing!
The irony of the ‘healthcare rationing’ critique is that our current system already has significant levels of healthcare rationing. Anytime someone doesn’t buy health insurance or has inadequate health insurance coverage because of high premiums, that is a textbook example of healthcare rationing.
The challenge for Medicare-for-All will be predicting the initial surge in utilization rates with the rollout of Medicare-for-All, as people start getting the basic and preventive care they chose not to receive under the private insurance-based system. In the long-run, higher utilization rates will save money as people get more preventive care services and address potentially expensive health issues earlier in their development.
Second, Medicare-for-All isn’t socialized medicine. The doctors, nurses, hospitals, clinics, pharmaceutical companies, and medical equipment manufacturers all remain in the private sector under Medicare-for-All. Only the administrative function for U.S. healthcare, currently handled by private insurance, will be rolled into the public sector. A patient under Medicare-for-All is unlikely to ever talk to a public employee during a treatment or service delivery. Medicare-for-All is statism, but not socialism. The British National Health Service is socialized medicine.
It is too complex!
This is my favorite complaint about Medicare-for-All, especially coming from Democrats proposing a public option and other tweeks to Obamacare. On the day it was passed, ACA contained 2,300 pages and would soon include over 16,000 more pages in additional rules and regulations. The section of the Social Security Act of 1965 creating Medicare contained only 138 pages. Complex is the arcane, special interest laden maze that Obamacare has grafted onto our system. Medicare-for-All simplifies everything by blowing all that up, leaving us with a familiar healthcare system under Medicare that is already established and functioning.
Medicare-for-All proponents need to address rational ignorance
Unfortunately, the portrayal of Medicare-for-All as radical reform is, in part, due to Sanders himself and how he sells the idea to Democratic voters — who generally support the concept, even among many of Sanders’ non-supporters.
“If you support Medicare-for-All, you have to be willing to end the greed of the health insurance and pharmaceutical industries,” Sanders says in his current stump speech. “That means boldly transforming our dysfunctional system by ending the use of private health insurance. It is imperative that we remain steadfast in our commitment to guarantee healthcare as a human right and no longer private corporations to make billions of dollars in profits off Americans’ healthcare.”
Drama sells and Sanders understandably presents his healthcare proposal in that light. But while bold rhetoric may work for Democratic activists, it may be counterproductive in persuading those on the fence with respect to Medicare-for-All.
Before he died, Fox News analyst Charles Krauthammer conceded that this country was heading towards a Medicare-for-All system. He wasn’t a fan, even as he acknowledged its legitimate political attraction.
“I think, historically speaking, we’re at the midpoint,” he told Fox News’ Chris Wallace in May 2017 as Congress was debating whether to end Obamacare. . “We had seven years of ObamaCare, a change in expectations, and I would predict in less than seven years we’ll be in a single-payer system.”
Predicting that whatever Congress and President Trump came up with in 2017 would be ‘rickety,’ Krauthammer concluded: “It’s likely that Republicans are going to suffer at the polls, and as a result of that — if that happens — you’re going to get a sea-change in opinion. Then there’s only two ways to go: to a radically individualist system, where the market rules, or to single-payer. And the country is not going to go back to radically individualist.”
Unlike Joe Biden or Pete Buttigieg or Kamala Harris, Krauthammer educated himself on single-payer systems (e.g., Medicare-for-All). He consciously went beyond rational ignorance, though he remained a critic of the statist approach to healthcare. The radical approach to healthcare is our current private insurance-based, individualist system. It has failed and Krauthammer grudgingly acknowledged as much.
Medicare-for-All is the prudent expansion of a well-established program to other segments in the population that are, on average, healthier than those currently covered by Medicare. The overall cost effectiveness of Medicare should increase as it covers younger, healthier population segments.
In truth, Medicare-for-All is the most prudent, safest, and least complicated way to bring meaningfully improvement to the U.S. healthcare system. Tinkering on the margins by offering a public option (of unknown price competitiveness) within an already bloated, inefficient healthcare system is far costlier and riskier.
K.R.K.
Comments and suggestions can be send to: kroeger98@yahoo.com
Growing up in America’s farm belt, weather proverbs were commonly heard and taken seriously. The one I always remember I first heard from my grandmother: “Frogs croaking on the lake, means an umbrella one must take.” Or something like that.
She didn’t live near a lake, so I’m not sure how useful that piece of folk wisdom was for her, but it stuck with me. And, as it turns out, the proverb has some basis in fact. Frogs do croak more on hot, humid days — which is a good predictor of stormy weather.
But the way my grandmother used the proverb, or at least how my child’s mind interpreted it, I believed for years that croaking frogs caused thunderstorms. Croaking frogs, of course, do not have such power.
Years later, I would realize my grandmother offered me my first lesson in spurious correlations, and I’ve used the croaking frogs proverb in statistics classes many times since.
The lesson is one most people hear many times during their education: Correlation is not causation. Two events (x and y in the graphic below) can be statistically correlated but not be causally related, as they are both impacted by the true causal factor (z).
Frogs are affected by the same forces — temperature, humidity and air pressure — that cause thunderstorms. There is no causal relationship. To this day, I still call these relationships croaking frogs.
We may have a new example of this inferential deficiency concerning an analytic question of current importance: Did meddling by Russia’s Internet Research Agency(IRA) impact the final outcome of the 2016 election?
Four University of Tennessee researchers, Damian J. Ruck, Natalie Manaeva Rice, Joshua Borycz, and R. Alexander Bentley, have concluded, based upon a time-series analysis of IRA tweets and their diffusion within the Twittersphere during that election, that IRA Twitter activity predicted the 2016 election results. In their study released in July, they concluded:
“We find that changes in opinion poll numbers for one of the candidates were consistently preceded by corresponding changes in IRA re-tweet volume, at an optimum interval of one week before. In contrast, the opinion poll numbers did not correlate with future re-tweets or ‘likes’ of the IRA tweets. We find that the release of these tweets parallel significant political events of 2016 and that approximately every 25,000 additional IRA re-tweets predicted a one percent increase in election opinion polls for one candidate. As these tweets were part of a larger, multimedia campaign, it is plausible that the IRA was successful in influencing U.S. public opinion in 2016.”
The Washington Post’s Philip Bump wasted no time in challenging the Ruck et al. study for its failure to account for other causal factors that may have acted on both IRA Twitter activity and Trump’s public support:
“It’s important to note that the researchers focused on retweets and not overall tweets from the IRA. (In fact, they found that “we see weak evidence for an effect in the opposite direction, suggesting the possibility that IRA Twitter activity is increasing in response to Trump’s polling.”) This suggests that, if there was a meaningful correlation between Twitter activity and poll data, both were driven by some outside engagement. People becoming active on Twitter also may have happened as they were demonstrating more support for Trump. This is what’s known as a causal fork: Both the IRA retweets and Trump support may have been caused by the same external thing. If there’s a correlation here, that is. Which is . . . up for debate.”
Bump also noted that the magnitude and targeting of IRA’s Twitter and Facebook activity was not large or precise enough to plausibly move public opinion:
“It’s important to note that, on its face, the idea that 25,000 retweets could drive national political polls by a percentage point seems highly unlikely. Over the course of the 2016 election, there were 75 million tweets directly related to the election itself. If only 1 percent of those were retweeted 10 times, that means that the 25,000 retweets are fitting into a flood of 75 million original and 7.5 million retweeted tweets. It means, in other words, that the requisite 25,000 retweets make up 0.03 percent of all of that Twitter activity.”
“There’s very little evidence that Russia effectively targeted American voters with messages that powered Trump’s victory. Russia paid for a lot of Facebook ads in the populous states of New York and Texas in the last five weeks of the campaign, but its ads targeting the three states that handed Trump the election — Michigan, Pennsylvania and Wisconsin — were seen by only 1,000 people. There’s no evidence at all that Russia used Twitter to target people in particular places or demographic groups, targeting that would have left fingerprints in the form of receipts for payment.”
To the credit of the University of Tennessee researchers, they acknowledged the limitations of their study when they write, “Causation is not proven by this analysis, but certain directions of causality can be ruled out when one time series does not predict the other…We take the view that IRA Twitter activity was representative of a larger, multimedia disinformation campaign.”
Ruck et al. also write that their intent was to test “prediction, not causality,” as they admitted it is unlikely that “25,000 retweets could influence one percent of the electorate in isolation.” And, most appropriately, they recognize their study cannot rule out the importance of unmeasured factors that could render their findings spurious. They write in the study’s concluding section:
“Any correlation established by an observational study could be spurious. Though our main finding has proved robust and our time series analysis excludes reverse causation, there could still be a third variable driving the relationship between IRA Twitter success and U.S. election opinion polls. We controlled for one of these — the success of Donald Trump’s personal Twitter account — but there are others that are more difficult to measure; including exposure to the U.S domestic media.”
This is where the Ruck et al. research makes its biggest analytic error. What they call the ‘third variable’ is probably a set of variables — unmeasured and uncontrolled for in the Ruck et al. study — that, had they been included in the study, would likely washout the statistical significance of the IRA retweets.
By the Mueller investigation’s own estimate, IRA spent $100,000 between 2015 and 2017, with only $46,000 dedicated to Russian-linked Facebook ads purchased prior to the 2016 election. According to freelance journalist Aaron Maté, “That amounts to about 0.05 percent of the $81 million spent on Facebook ads by the Clinton and Trump campaigns combined — which is itself a tiny fraction of the estimated $2 billion spent by the candidates and their supporting PACS.”
There is, however, an obvious candidate for the honor of being the “larger, multimedia disinformation campaign” Ruck et al. consider as the more likely driving force behind the “manipulation” of the 2016 electorate. That third variable is the Trump campaign’s social media campaign, powered by Cambridge Analytica’s massive data warehouse, which included data harvested from over 50 million Facebook user profiles.
Unlike IRA’s use of Twitter and Facebook, where the hard evidence shows little sophistication in both content and targeting, Cambridge Analytica engineered one of the most sophisticated Big Data-driven social media campaigns in presidential history.
In an interview with CNBC, the 2016 Trump campaign’s digital director, Brad Parscale, detailed how his team, including Cambridge Analytica, created highly targeted Facebook advertising based on scientific testing to optimize each advertisement’s click rate. “We were making hundreds of thousands of them (ads on Facebook) programmatically. … (On an) average day (we would make) 50,000 to 60,000 ads, … changing language, words, colors, changing things because certain people like a green button better than a blue button, some people like the word ‘donate’ over ‘contribute,’” Parscale told CNBC.
Just on scale, IRA’s efforts pale in comparison to Parscale/Cambridge Analytica’s. Add to that the much higher level of campaign sophistication by Parscale/Cambridge Analytica, and it begs the question, how could any serious research on the impact of Russian meddling in 2016 not include measures of the Trump’s campaigns social media efforts (and Hillary Clinton’s as well for that matter)?
Ignoring Cambridge Analytica’s social media campaign, Ruck et al. have given us a croaking frog-level analysis. It is as if the Ruck et al. research team, while sitting in a small row boat on a lake, experienced a large wake and attributed it to an 8-meter motor boat passing by, ignoring the fact that a 100-meter, 6,700 gross tonnage yacht passed by at the exact same time.
While their forthrightness on their study’s flaws is admirable, Ruck et al. have not done the measurements and work necessary to release any meaningful results on a subject as politically volatile as Russia’s influence on the 2016 election. As it stands today, their study offers little to the conversation.
K.R.K.
Comments and criticisms can be sent to: kroeger98@yahoo.com
The original intent behind federally-mandated desegregation busing was noble: ‘Separate but equal’ was not working for many African-American students in the 1950s and 60s. Busing policies were designed to improve the educational opportunities of African-American children by integrating them systematically into predominantly white school districts.
The desegregation busing concept was predicated upon research conducted in the 1960s, specifically the Coleman Report published in 1966. In that study, including more than 150,000 students, it was found that learning within mixed-race classrooms was more important to the academic achievement of socially disadvantaged African-American children than was per-pupil funding.
According to the researchers, it wasn’t enough to improve funding to schools in economically disadvantaged school districts. The students in these districts would achieve better educational outcomes if they were educated in predominantly white school districts.
But it took the 1971 Supreme Court ruling in Swann v. Charlotte-Mecklenburg Board of Educationto provide the final impetus for desegregation busing to advance nationwide. In ruling in favor of Swann, the Supreme Court decided that for a school district to achieve racial balance it meant redrawing school boundaries and the use of busing in that aim was a legitimate legal tool.
So began the liberal project to integrate the American school system through federally-mandated (forced) busing. In the 1970s, busing designed to desegregate mostly urban school districts began. School districts in Boston (MA), Kansas City (MO), Las Vegas (NV), Los Angeles (CA), Nashville (TN), Prince George’s County (MD), Richmond (VA), and Wilmington (DE), among others, instituted mandatory busing where a select number of students were assigned and transported to racially segregated schools.
Reducing racial segregation in public schools became a federal requirement following the Supreme Court’s 1954 ruling in Brown v. Board of Education, but, for many reasons, mandatory busing did not achieve this goal.
From 1972 to 1980, despite desegregation busing in many urban school jurisdictions, the percentage of blacks attending mostly-black schools barely changed, moving from 63.6 percent to 63.3 percent, noted David Frum in his 2000 book, How We Got Here: The 1970s (The Decade That Brought You Modern Life — For Better Or Worse).
As to the impact of busing on academic achievement, a 1992 Harvard study found no discernable improvement among black and Hispanic students as a result of court-ordered busing.
Busing did, however, leave a political mark, especially on liberal Democrats who had championed the policy since its inception. Many white families whose children were bused to predominately African-American schools resented the government’s intrusion. For many families, the quality of local neighborhood schools was a major factor in deciding where to buy or rent a home. Children selected for busing programs often had to travel more than an hour to get to school, though, in many cases, their neighborhood school was within walking distance.
Public Opinion on Busing in the 1970s
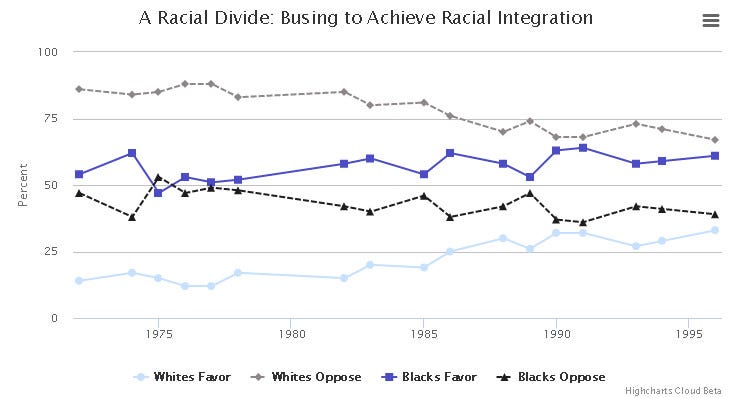
Public opinion data collected between 1972 and 1996 by the National Opinion Research Center (NORC) shows the level of discontent among whites with respect to busing was always high (see Figure 1).
In the 1970s, while African-Americans were evenly split in their support for busing, whites opposition to the policy never fell below 75 percent. Public opinion on busing has changed little since 1996 (the last year NORC asked a busing question on its General Social Survey [GSS]). A more recent 2007 poll conducted by the Pew Research Center found that 59 percent of Americans would prefer that students stay in their local schools, even if that meant most students would be of the same race.
Figure 1: Public attitudes over time regarding mandatory busing
Amid other social issues that dominated politics in the 1970s (e.g., abortion, prayer in school, the Equal Rights Amendment, etc.), few were as potent as busing. In his 1980 presidential campaign, Ronald Reagan told the Sacramento Press Club:
“Federal control of education has become a reality. If I am elected President it would be my intention to issue strict instructions to the Department of HEW and other federal departments to get off the back of state and local school systems, to leave the setting of policies and the administration of school affairs to local boards of education.”
When Reagan won the 1980 election, many attributed his victory, at least in part, to the public’s opposition to federal programs such as busing. And it was within this political environment that then U.S. Senator Joe Biden (DE) actively worked with some southern Democrats, including avowed segregationists, to end federally-mandated busing. At the time, Biden supported the concept of school desegregation, but not the use of federal directives to do so. Though not a southern state, Delaware’s electorate (while friendly to Democrats) shares some conservative attitudinal characteristics with many southern states, enough so that Biden’s political career might have derailed prematurely had he not publicly opposed federally-mandated busing.
A yes-vote on busing in the mid- to late-1970s might well have ended Biden’s Senate career with the 1978 Senate race — part of a national election where five Democratic incumbent Senators lost their seats: Floyd Haskell (Colorado), Dick Clark (Iowa), William Hathaway (Maine), Wendell Anderson (Minnesota), and Thomas McIntyre (New Hampshire).
To attack Biden in 2019 over a policy position he took in 1977 that was both defensible on merit and popular with his Delaware constituents is cynical by even modern political standards.
Is Support for Busing Trending Up?
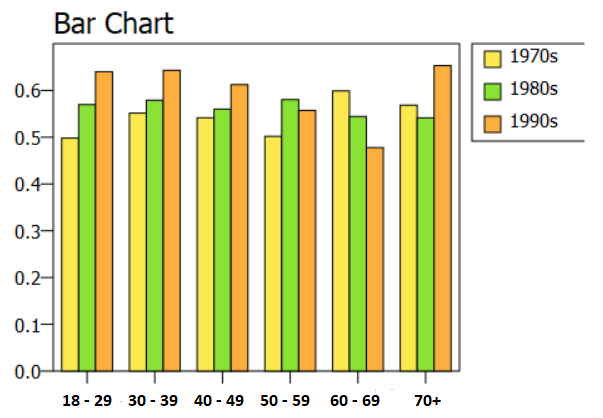
If we accept the polling numbers at face value, public support for busing trended upwards after the tumultuous 70s, particularly among young African-Americans and whites (see Figures 2 and 3). Support among African-Americans between 18 and 29 years old rose from 50 percent in the 1970s to 65 percent in the 1990s; among whites, support grew significantly in all age groups, though never exceeding 50 percent for any single group.
Figure 2: African-American attitudes regarding busing by age and decade
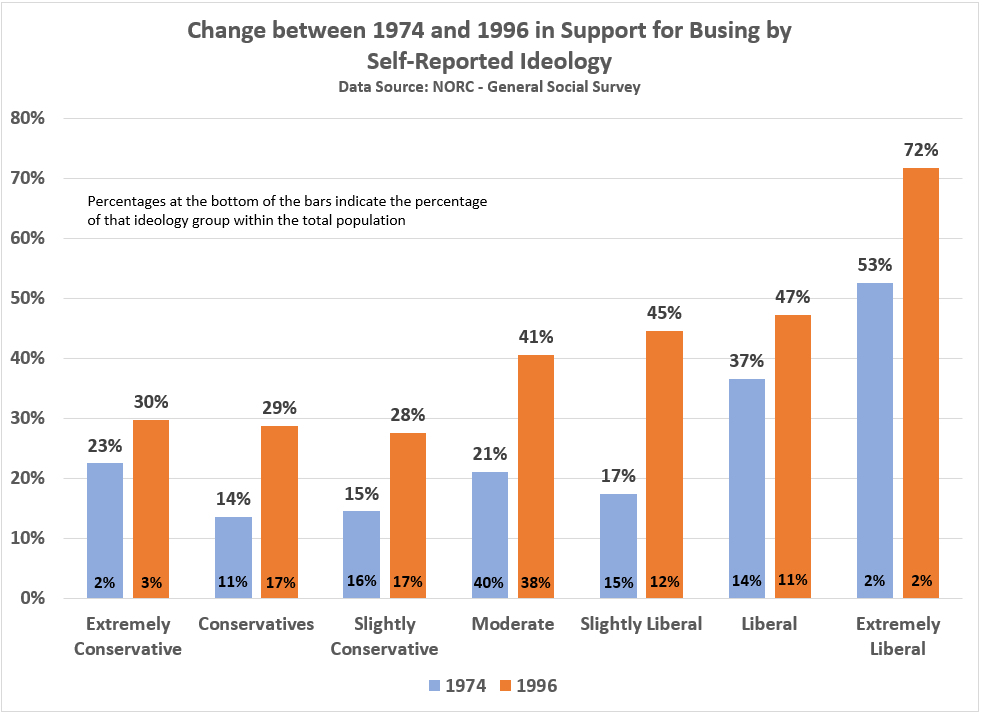
The positive trend in busing support even extended across ideological groups (see Figure 4). For ‘extremely liberal’ GSS respondents, which make up about two percent of the U.S. adult population, support for busing grew from 53 percent to 72 percent.
At the other end, ‘extremely conservative’ Americans, accounting for two to three percent of the U.S. adult population, support for busing increased from 23 percent to 30 percent between 1974 and 1996.
Among a more populous segment of the population, moderates, support for busing nearly doubled from 21 percent to 41 percent.
Figure 4: Change in Attitudes Towards Busing by Ideological Group (1974 to 1996)
Granted, 1996 is over 20 years ago. A lot can change; but as pointed out, a 2007 Pew Research found similar attitudes regarding busing. A majority of Americans prefer children going to their neighborhood schools, even if that means they will not experience as much ethnic and racial diversity during their education. This finding is not controversial. Most parents prefer their children to go to their neighborhood schools — even as there are parents that are willing to bus their children to schools that offer opportunities their neighborhood school may not offer (e.g., music, sports, advanced math/science, cultural diversity, etc.).
As many mandated busing programs either being discontinued or transitioned to voluntary programs through the 1990s, the visceral component to the public’s opposition to federally-mandated busing waned. Moreover, by the 1990s, fewer and fewer Americans had personal experiences with the busing controversies of the 1970s. Temporal distance does make the heart grow fonder in this case.
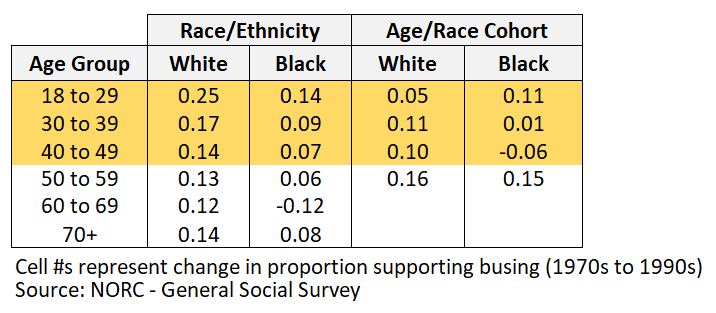
Yet, the residual effects of the 1970s are still evident in the polling data from the 1990s. Using the numbers from Figures 2 and 3 (above), the change in the proportion of respondents supporting busing from the 1970s to 1990s is reported in the first two columns in Figure 5. Again, the biggest increases in support for busing occurred among white and younger Americans — demographic groups in the 1990s least likely to have firsthand experience with the controversies surrounding busing in the 1970s.
However, if we observe the age and race cohorts, we see indications that those memories lingered with those who most likely experienced — directly or indirectly — busing in the 1970s, particularly among African-Americans. For example, the cohort of African-Americans who were 30 to 39 years old in the 1970s — an age most likely to have small children in a public school system — were 50 to 59 years old in the 1990s. This cohort’s support for busing increased one percentage point from the 1970s to 1990s (not statistically significant). Among the cohort of African-Americans between 40 to 49 years years old in the 1970s — an age segment most likely to have older children in a public school system — support for busing actually declined six percentage points by the 1990s.
Figure 5: Change in Attitudes Towards Busing by Age/Race Cohorts (1974 to 1996)
Do the Democrats Really Want to Bring Back Mandated Busing?
Federally-mandated busing was a traumatic experience for many parents and children, black and white, even if there are cases such as entrepreneur Robert F. Smith where the experience brought positive results to their lives (Note: Senator Kamala Harris participated in a voluntary busing program in Berkeley, California — a policy Joe Biden does not oppose).
More pointedly, federally-mandated busing didn’t work. In the aggregate, it didn’t improve the academic performance of African-American children bused to mainly white schools, nor did it lead to a significant drop in school segregation. But it did create massive amounts of resentment towards the federal government.
As a federally-mandated program, the entire enterprise failed.
But that hasn’t stopped political opportunists today from casting judgment on those that lived through busing controversy in the 1970s.
The Nation’s Jonathan Kozol offers an ahistorical rebuke of Joe Biden’s political positioning on busing in the 1970s, using the very real plight of African-American parents that know their children will not get the education they deserve if they can only attend an inner city school, suggesting to his readers that Biden was nothing less than a closet sympathizer with racists:
“As the mainstream media repeatedly reminds us, Biden is a likable man in many ways. Even his critics often speak about his graciousness. But his likability will not help Julia Walker’s grandkids and her great-grandchildren and the children of her neighbors go to schools where they can get an equal shot at a first-rate education and where their young white classmates have a chance to get to know and value them and learn from them, as children do in ordinary ways when we take away the structures that divide them.”
Kozol’s admirable tenure teaching fifth grade for two years in Boston’s suburban interdistrict program, the longest-lasting voluntary integration effort in the nation, turns out to be further evidence that experience does not equate to knowledge or wisdom.
“Regardless of Biden’s intent, he was among the politicians who successfully surfed the surge of anti-busing populism. This wave included parents who were horrified by overt racism, but who opposed putting their children on buses. And this wave also included avowed racists and opportunists who, in their opposition to busing, hid behind self-righteous platitudes.”
Biden wasn’t representing his constituents, he was cynically ‘surfing’ the issue so as to not anger overt and closet racists, implies Blume.
Only Chairman Mao has achieved such moral and ideological purity as Messrs. Kozol and Blume, whose unexamined platitudes on race and segregation offer little substance to build an actual policy around. That federally-mandated busing hurt the cause of ending school segregation is beside the point to today’s social justice vanguard. That voluntary busing programs achieve better results than federally-mandated programs ever did is also inadmissible. Uncle Joe must be shame-punished, sans evidence or reason.
To Biden’s credit, he hasn’t backed down on how he explains his busing position in 1977. But he will. It is only a matter of time before he apologizes for not being properly enlightened back in the day. He’ll come to Jesus and all will be good until he again says something racially insensitive or awkward [Note: The Biden campaign speechwriter(s) responsible for Biden’s most recent ‘kid wearing a hoodie’ comment need(s) to be fired. If the writer is Biden, himself, well…]
Very few political writers and Democratic party operatives were alive during the 1970s, much less experienced the social upheaval federally-mandated busing caused. They would well-advised to talk to people that lived through it from all perspectives — positive and negative. Their own perspective might change as a result.
But if a new federally-mandated busing initiative to integrate America’s public schools is what they want, good luck to any 2020 Democratic candidate willing to run on that idea. They’ll need it.